|
Literacy levels are increasingly important in health care because professional nurses and other health care professionals often use written health education materials as a major component in patient education. In South Africa, no current instrument is available to assess the literacy levels of patients in the primary health care setting, though several instruments have been developed and validated internationally. The purpose of this paper was to adapt and validate the Rapid Estimate of Adult Literacy in Medicine Revised (REALM-R) to the South African context. The REALM-R is a short instrument that is designed to rapidly screen clients in the primary health care setting for low health literacy. A modified Delphi-technique was used to measure the judgement of a group of experts for the purpose of making a decision. Eight experts in the field of Nursing Science were selected purposively to obtain the most reliable consensus. Data was collected by means of a self-report whereby participants responded to a series of questions posed by the researcher. Descriptive statistics was used for analysing data. The REALM-R was adapted to the South African context to ensure that the literacy level of South African clients is measured with an appropriate instrument.
Geletterdheidsvlakke word toenemend belangrik in gesondheidsorg aangesien geregistreerde verpleegkundiges en ander gesondheidswerkers dikwels geskrewe gesondheidopvoedkundige materiaal gebruik. Op die oomblik in Suid-Afrika is daar geen geletterdheidsvlaksinstrument beskikbaar om pasiënte in primêre gesondheidsorg se geletterdheid te toets nie. Daar bestaan wel gevalideerde internasionale instrumente. Die doel van die studie was om die REALM-R, ‘n internasionaal gevalideerde mediese geletterdheidsinstrument, aan te pas en te valideer om in die Suid-Afrikaanse konteks gebruik te kan word. Die REALM-R is ‘n kort geletterdheidsinstrument wat ontwikkel was om primêre sorg pasiênte wat moontlik lae geletterdheidsvaardigheid het, te kan sif. ‘n Aangepasde Delphi-tegniek is gebruik om die oordeel van ‘n groep kundiges in te win. Agt kundiges in verpleegwetenskappe is doelgerig gekies ten einde ‘n betroubare ooreenkoms te verkry. Data is deur middel van self-raportering ingewin deurdat die deelnemers op vrae, gestel deur die navorser, geantwoord het. Beskrywende statistiek is gebruik om die data te ontleed. Die REALM-R is aangepas vir die Suid-Afrikaanse konteks ten einde ‘n geskikte instrument beskikbaar te stel om die geletterdheidsvaardigheid van primêre sorg pasiente vinnig en akkuraat te kan meet.
Background and rationale
The Rapid Estimate of Adult Literacy in Medicine Revised (REALM-R) is rapid-screening instrument that is used to assess how well primary health care patients read words that they commonly come across in the primary health care setting (Bass, Wilson & Griffith 2003:1037). The REALM-R is designed to identify clients that have potential literacy problems. According to Bass et al. (2003:1036), the REALM-R is a medical word recognition and word pronunciation test which consists of 8–11 commonly used medical words. Leipzig (2001) indicates that in order for a person to make meaning of printed words, the person must be able to identify the words in print. The process is called word recognition. The author states that a person must also be able to understand or comprehend the meaning of the words. Word recognition and comprehension therefore form an integral part of reading printed information such as written health education materials. The REALM-R, however, is only a word recognition tool and does not measure reading comprehension (Health literacy assessment tool 2006). Patients in primary care clinics or persons needing health education are asked to read the list of medical terms. Any word that is mispronounced or not attempted is considered as an error. Each word pronounced correctly is marked as such. If the participant has a score of less than 6 out of 8, the participant can be considered at risk for low literacy (Feinberg & Pharmd 2006). The test can be administered in less than 2 minutes; it is ideal for being adapted and validated for the South African context. The REAM-R is validated in English and makes use of only readability testing to determine the patient’s health literacy levels. Low literacy refers to the inability to read, write or use numbers effectively (Weiss 2007:8). The National Adult Literacy Survey (Kirsch, Jungeleut & Jenjins 1993) indicates that 48% of American adults do not have theliteracy skills necessary to functioning adequately in the society. In South Africa, Skill Share International (2000) found that one in six people (40%) are functionally illiterate. Literacy levels become increasingly important in the health care context, because professional nurses and other health care professionals often use written health education materials as a major component for patient education. Health education materials often require reading levels higher than the reading level of a large portion of the South African population people (Fisher 1999:56). Patients with low literacy will have difficulty understanding health care instructions and making appropriate health care decisions (Boswell, Cannon, Aung & Eldrige 2004:61). Boswell et al. (2004:61) observed that health education materials are often prepared at the level of the eighth grade or higher and therefore the most commonly used materials would not meet the needs of the low-literate person. The 2001 census in South Africa indicated that 51% of South Africans aged 20 and older should be able to understand patient information if a grade 7 reading level is used (Statistics South Africa 2001). The percentage has increased to 66% with the household survey in 2004 (South Africa, Statistical release P0318 2004). However, the Department of Health (2005:60) acknowledges that more than 8 million South Africans may not benefit from health promotion materials currently used in primary health clinics and hospitals. The limited ability to read and understand health care instructions directly translates into poor health outcomes (Weiss 2007:13). The relationship between low literacy and adverse health outcomes is represented by two underlying processes. Firstly, low literacy may have a direct negative effect on health due to the barriers to accessing information and using health information. Secondly, low literacy can be a marker for other conditions such as poverty and lack of access to health care that may lead to poor health (Pignone et al. 2005). In South Africa, no current instrument is available to assess literacy levels of patients in the primary health care setting, as compared to several instruments developed and validated internationally.
Definition of main concepts
The definitions for the study are as follows: • Functional health literacy refers to the ability to perform basic reading tasks that are required to function in the health environment (Pawlak 2005:174). • Health education materials are described as health education materials that are the health promotion measures or materials used to encourage healthy behaviour and promote health (Naude & Setswe 2000:105). They are aimed at giving people knowledge in order to understand and act to improve their own health. • Health literacy is the degree to which an individual has the capacity to process and understand basic health information and services needed to make appropriate health decisions (Pignone et al. 2005:185). The World Health Organization defines health literacy as the cognitive and social skills that determine the motivation and ability of individuals to gain access to, and to understand and use, information in ways that will promote and maintain good health (Scudder 2006:31). • Illiteracy is described by Rivas (1997) as the inability of an individual to read, write or use computational skills in every day life. • Literacy can be defined as an individual’s ability to read, write and speak, to compute and solve problems at levels of proficiency necessary to function in an occupation or in society, to achieve one’s goals and to develop one’s knowledge and potential (Berkman et al. 2004). • Literacy assessment tool is defined as an assessment tool used to evaluate literacy and health literacy. Such tools may be categorised as word recognition tests, reading comprehension tests and functional health literacy tests (Andrus & Roth 2002:282).
Research problem and purpose of the study
The impact of low literacy in health care settings in South Africa is not clearly understood. The lack of suitable instruments creates a vacuum in the knowledge base. Though several databases were searched and intensive contact made with the Medical Research Council and the Human Sciences Research Council as well as other universities, no literacy-specific instrument validated in the South African context could be found. The research question posed to participants was: which modifications should be made to the REALM-R to adapt the current instrument to the South African context? The purpose of the study was to adapt and validate a suitable literacy instrument to measure the English literacy levels in primary health care patients. The aim was to adapt the REALM-R to the South African context.
Pawlak’s Health Literacy (Pawlak 2005:173) and the Adult Education Theory (Doak, Doak & Root 1996) were used as the theoretical bases for the research to assess the literacy levels of clients in the community care sector. Pawlak’s Health Literacy Model indicates that low health literacy has a number of adverse outcomes which may include poor health status, a lack of knowledge of health, a poor use and understanding of health care services, poor compliance to medication and treatment, increased hospitalisation and increased health care costs (Pawlak 2005:173). Literacy is considered to be the main determinant of health. A number of determinants influence health literacy such as genetics, level of education, socio-economic status, physical environment and social environment (Pawlak 2005:174). The determinants may be viewed individually or together with other determinants. If the level of health literacy improves, the level of care will be matched with the need, the communication between the health care user and provider will be improved, the consumer will be informed and treatment compliance will improve. The outcome will be reduced health disparities and improved health. Without improving the health literacy of the whole community, health on a population level will not improve.The Adult Education Theory is concerned with teaching adults with low literacy (Doak, Doak & Root 1996:1).
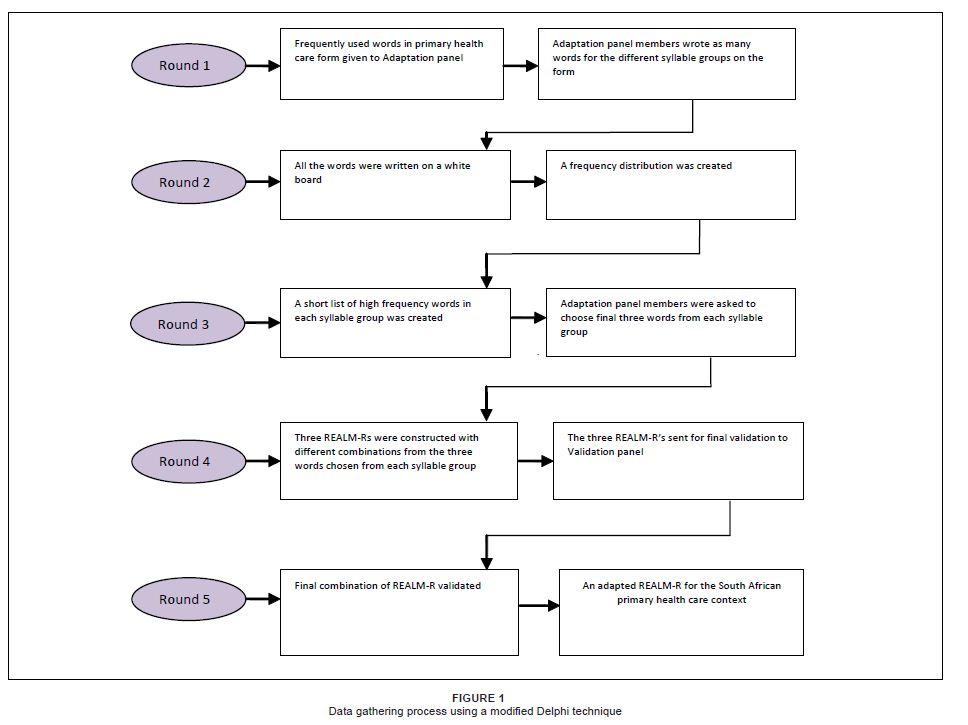 |
Figure 1: Data gathering process using a modified Delphi technique
|
|
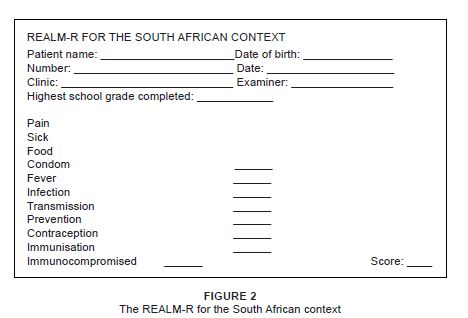 |
Figure 2: The REALM-R for the South African context
|
|
|
Research method and design
|
|
The research methods and design for the study were as follows:
Research design
The Delphi technique was used to identify the words for the REALM-R adapted for the South African context. Participants were together during data gathering and they reached consensus in a relatively short time. Similarly, Whitehead (2008:891) used the Delphi technique for examining the health promotion and health education in nursing practice and nursing education where the technique was found suitable. A modified Delphi-technique (Figure 1) was used to obtain the judgement of a group of experts for the purpose of making a decision (Burns & Grove 2005:16). Using the Delphi-technique facilitated the reaching of a consensus among experts who have different views and perspectives. The technique enables group problem-solving by using a process of problem definition, discussion, feedback and revision (Modified Delphi Technique [n.d.]). The Delphi technique was modified for this study as two panels were used. The Adaptation panel, chosen to change the American words to words more suitable for the South African context, was together in one room and the various rounds of data gathering occurred in a single meeting. The second panel, the Validation panel, a larger panel that included all the members of the Adaptation panel, was contacted via email.
|
Table 1: Words chosen by panel of experts according to the number of syllables; frequency in brackets
|
|
Table 2: Three words per syllable group with the highest frequency chosen for the adaptation
of the REALM-R
|
|
Table 3: http://hsag.co.za/index.php/HSAG/article/downloadSuppFile/468/470
|
Population
Two panels were constituted, an adaptation panel who participated in the adaptation of the REALM-R to the South African context. A second panel, the validation panel, was used to validate the newly constituted South African REALM-R. The Adaptation panel comprised of experts in the field of Nursing Science in order to obtain the most reliable consensus. Members of the panel were chosen if they were willing to participate and had any of the following health-promotion expertise: primary health care, community health, oncology and palliative care, health promotion and nursing research qualifications. The sampling method was purposive and convenient as the participants were chosen for their expert knowledge and availability in the Tswane area. Eight experts were selected to participate in adapting the REALM-R for the South African context. Thangaritaman and Redman (2005:120) indicate that the panel size can range from 4 to 3000 experts. The outcome of the work done by the Adaptation panel were three possible versions of the South African REALM-R. The validation panel was used to determine the face and content validity the adapted South African REALM-R. The validation panel included all the members of the adaptation panel as well as a wider selection of registered professional nurses’ expertise in community health, primary health care and health promotion. The second panel comprised of 30 participants. The criteria for inclusion were expertise in health promotion, availability through electronic means (email or fax) and willingness to participate.
Data gathering
The data gathered were guided by the original REALM-R. According to Bass, Wilson and Griffith (2003:1037), the REALM-R is an instrument designed to identify how well primary care clients understand words that are commonly used by the physicians or other medical staff. The test consists of eight words which the person must read out loud. There are three additional one syllable words to familiarise the person with the test and to put the person at ease. The REALM-R (South Africa) was based on REALM-R (US) with regard to the number of words and the number of syllables of the different words. Before the data gathering, detailed information was given to each member of the panel on the REALM-R. Each member also received a copy of the original REALM-R (US) to allow them to view the format of the REALM-R. Data were collected by means of self-report where the panel members responded to a series of requests posed by the researcher (Polit & Beck 2008:324). A form was created, the Frequently Used Words in Primary Care form. The form was divided in six columns, with column headings: One syllable, Two syllables until the last column requiring words with six syllables. The steps followed in data gathering were: • Round 1 (Adaptation panel): the purpose of Round 1 was to obtain as many suggestions as possible from the panel (Thangaratinam & Redman 2005:121). In Round 1, the designed form was given to each member of the panel of experts. The panel of experts was asked to list as many words as possible for each of the syllable groups on the form. The results are displayed in Table 1. • Round 2 (Adaptation panel): participants were asked to evaluate each idea (Modified Delphi technique, [n.p.]). In Round 2, all the words chosen by the experts were listed on the white board and a frequency distribution was created. • Round 3 (Adaptation panel): the experts were then asked to individually choose the words from each syllable group that they considered most appropriate for the REALM-R (South Africa). The participants were asked to list the words in order of importance. In Round 3, the second round words chosen were listed and a shortlist was created. The experts were again asked to choose individually, from the remaining words, the three most appropriate words for each syllable group. The final list was compiled (Table 2). • Round 4 (Validation panel): [i]n Round 4, the researcher constructed three REALM-Rs with different combinations of the words identified by the Adaptation panel. The three REALM-Rs were then sent to the Validation panel who had to validate the most appropriate version of the South African REALM-R. • Round 5 (Researcher): A frequency distribution was done again on the number of times each of the three proposed South African REALM-R was chosen. The REALM-R with the highest score was finally chosen for the South African context (Figure 2).
Data analysis
Descriptive statistics were used for data analysis. Descriptive statistics are usually presented in averages or percentages (Polit & Beck 2008:556). The data analysis was appropriate because in each round of the data gathering, as presented in Figure 1, a frequency distribution was done. The final REALM-R was also selected on the basis of the number of times it was chosen by the members of the Validation panel.
Adaptation of the REALM-R to the South African context
In the second round of the Delphi technique, a combined list and frequency distribution of the participants’ lists were created as indicated in Table 1. In Round 4, three possible South African REALM-R literacy instruments were constructed based on possible combinations of the words reflected in Table 2. The exact format of the original REALM-R was used for the adapted REALM-R for the South African context. Only the words of the original REALM-R were adapted for the South African context. The number of words and number of syllables of the words remained unchanged. The number of words and syllables were as follows: three words with one syllable, two words with two syllables, three words with three syllables, one word with four syllables, one word with five syllables and one word with six syllables. The final adapted REALM-R for the South African context was then used for assessing the literacy levels of primary health care clients in the West of Tshwane using the REALM-R. Figure 2 illustrates the REALM-R adapted for the South African context. Liepzig (2001) maintains that, in order for a person to make meaning of printed words, the person must be able to identify words in print. The author adds that word recognition forms an integral part of reading printed information such as written health education material. The advantage of assessing patient’s literacy levels in the primary health care clinic is that the REALM-R is easy to administer and takes only 2 min - 3 min, while minimal training is needed by the health care professionals. If the patient’s literacy level can be assessed before or during the consultation, the registered professional nurses will be in a position to adapt their health education strategies immediately and teach the patient on a level where learning can actually take place. Furthermore, the REALM-R is paper-based and no computer skills or any other particular skills are needed.
The REALM-R was adapted and validated for the South African context with the approval of the original developers (Bass, Wilson & Griffith 2003:1037). The Ethics Committee of Tshwane University of Technology also approved the proposal (# 2005/02/008). The participants were a group of experts and they signed imformed consent before participation in the study. Anonymity and confidentiality was ensured as no names were used during the data gathering procedures. Though the Adaptation panel were together in the room, each panel member participated individualy and they were requested to maintain the group confidentiality.
The validity and reliability of the South African REALM-R was ensured by the following measures. The United States REALM-R was validated as a shortened version of the REALM and was designed to be used in the public health sector and primary health care setting to identify patients with low literacy (Davis, Jackson, Mayeaurex, George, Murphy & Crouch 1993:1). The REALM-R correlates with a number of other tests including the SORT-R, WRAT-R, PIAT-R and the TOFHLA (Pawlak 2005:178). Table 3 indicates the correlation of the REALM-R with other literacy assessment tools according to the r-value. Davis et al. (1993:391) also indicate that the test–retest reliability of the REALM-R was 0.99. The Adaptation panel adapted the REALM-R for the South African context by choosing commonly used words when teaching or managing diseases or conditions in the primary health care setting. The validation panel was used to evaluate the instrument to ensure face and content validity. For this study, the consideration was whether the words were an adequate sampling of the various reading levels and if they were typical of the words used when teaching or managing diseases or conditions in the primary health care context in South Africa.
The members of the Adaptation panel were from the Tshwane area. The members from the Validation panel, though from a much wider context, did not represent all areas in South Africa. Further validation of the REALM-R in all the geographical areas in South Africa will be necessary before the REALM-R can be implemented throughout South Africa.
More research is needed to validate the REALM-R adapted for the South African context. The validation should include primary care patients speaking the other official languages in South Africa, not just Setswana.
Pawlak (2005:175) emphasises the central role of health literacy in improving a population’s health. Persons’ health literacy is dependent on their literacy level. The role of the registered professional nurse in achieving improved population health is therefore pivotal. Teaching in such a way that patients with low literacy cannot understand negates the purpose of teaching. Adapting the REALM-R to the South African context was therefore necessary to ensure that the literacy level of South African clients is measured with the appropriate instrument. Assessing a patient’s literacy level must become as normal as determining a patient’s temperature. Registered professional nurses must be taught to teach patients without depending on the written word. If the focus does not change, the burden of disease due to communicable and non-communicable disease in South Africa will continue unabated.
Andrus, R.M. & Roth, M.T., 2002, ‘Health literacy: A review’, Pharmacotherapy 22(3), 282–302. Berkman, N.D., Dewalt, D.A., Pignone, M.P., Sheridan, S.L., Lohr, K.N. & Lux L., 2004, Literacy and health outcomes, Evidence Report/Technology Assessment No. 87, Agency for healthcare research and quality, North Carolina. Bowling, A. & Ebrahim, S., 2005, Handbook of health research methods: Investigating, measurement and analysis, Open University Press, London. Burns, N. & Grove, S.K., 2005, The practice of nursing research, conduct, critique and utilization, 5th edn., Philadelphia, Saunders. Davis, T.C., Mayeaux, E.J., Fredrickson, J.A., Jackson, R.H. & Murphy, P.W., 1994, ‘Reading ability of parents compared with reading levels of paediatric patient education materials‘, Paediatrics 93, 460–468. Doak, C.C., Doak, L.G. & Root. J.H., 1996, Teaching patients with low literacy skills, 2nd edn., Philadelphia, JB Lippincott. Dreger, V. & Tremback, T., 2002, ‘Optimize patient health by treating literacy and language barriers‘, Association of operating room nurses 75(2), 280–293. Feinberg, J.L. & Pharmd, J.D., 2006, ‘Adult medication: Improving medication adherence in older adults’, viewed 12 February 2007, from http://www.adultmeducation.com Griffin, J., McKenna, K. & Tooth, L., 2006, ‘Discrepancy between older client’s ability to read and comprehend the reading level of written educational materials used by occupational therapists’, British Journal of Occupational Therapy 69(3), 144–145. Jackson, R.H., Davis, T.C., Bairnsfather, L.E., George, R.B., Crouch, M.A. & Gault, H., 1991, ‘Patient reading ability: An overlooked problem in health care’, Southern Medical Journal 84(10), 1172–1175. Kirsch, I., Jungelut, L. & Jenjins, L., 1993, Adult literacy in America: a first look at the National Adult Literacy Survey, DC, National Centre for Educational Statistics. Knowles, M., 1990, ‘Knowles’s Andragogy’, viewed 26 May 2007, from http://www.learningandteaching.info.htm Leipzig, D.H., 2001, ‘What is reading?’, viewed 12 January 2009, from http://www.readingrocket.org/article/352 Learning Ability Battery assessment tool for RPL, PLA & CASS administrator’s manual, 2005, 8th edn., Ferndale, Lead the field. Modified Delphi technique, n.d., viewed 27 July 2008, from http://www.communitydevelopment.uiuc.edu/modifieddelphitechnique Nath, C.R., Sylvester, S.T., Yasek, V. & Gunel, E., 2001, ‘Development and validation of a literacy tool for persons with diabetes’, The Diabetes Educator 27(6), Nov–Dec, 857–864. Naude, M. & Sewetse, G., 2000, Basic community health nursing, Sandton, Heinemann. Osborn, D., 2007, Language policy and language use in South Africa: an uneasy marriage, viewed 12 January 2009, from http://www.mail-archive.com/africanlanguages@yahoogroups.com/msg00524.html Pawlak, R., 2005, ‘Economic considerations of health literacy’, Nursing economics 23(4), 173–180. Pignone, M., De Walt, A.D., Sheridan, S., Berkman, N. & Lohr, K.N., 2005, ‘Interventions to improve health outcomes for patients with low literacy: A systemic review’, Journal of General Internal Medicine 20(2) Feb, 185–192. Polit, F.D. & Beck, C.T., 2008, Nursing research: Generating and assessing evidence for nursing practice, 8th edn., Philadelphia, Lippincott Williams & Wilkins. Quantitative management: introduction to the business world, 2003, Pretoria, University of South Africa. Rice, J.A., 2007, Mathematical statistics and data analysis, 3rd edn., University of California, Duxbury. Smith, J.L. & Haggerty, J., 2003, 'Literacy in primary care population: Is it a problem?', Canadian Journal of Public Health 94(6), 408–412. Steyn, A.G.W., Smit, C.F., Du Toit, S.H.C. & Strasheim, C., 2000, Modern statistics in practice, Pretoria, Van Schaik. Weiss, B.D., 1999, 20 Common problems in primary care, New York, McGraw–Hill. Weller, F.B., 1997, Bailliere’s nurses dictionary, 22nd edn., Philadelphia, Bailliere. Whitehead, D., 2008, ‘An international Delphi study examining health promotion and health education in nursing practice’, Journal of Clinical Nursing 17(7), 891–900.
|

